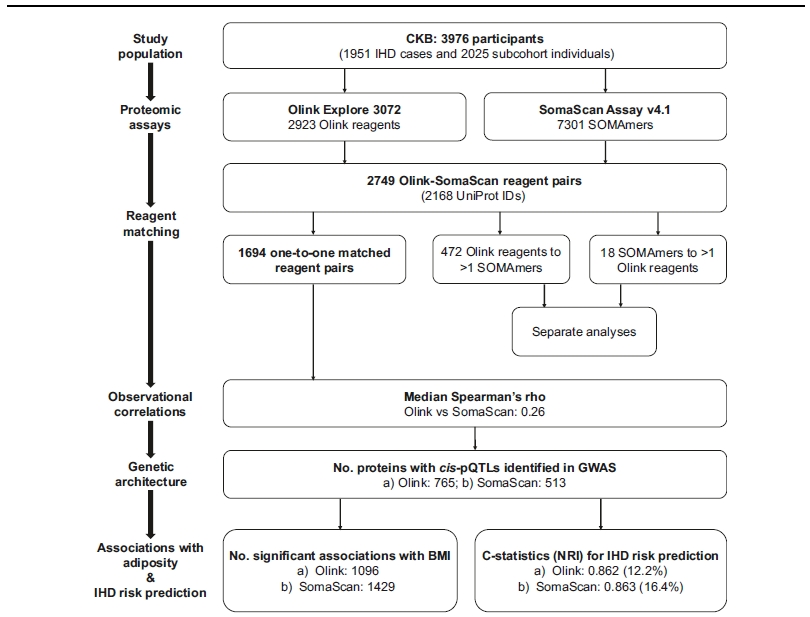
Fig. 1 | Summary of study design, analytical approaches, and key findings. Main analyses were conducted on 1694 one-to-one matched Olink-SomaScan reagent pairs in 3976 CKB participants. Results were corrected for multiple testing using false discovery rate within each platform. Risk predictionmodels for IHDwere built using conventional risk factors (age, sex, smoking, type 2 diabetes, systolic blood pressure, and waist circumference) and 1694 matched proteins. CKB China Kadoorie Biobank, IHD ischaemic heart disease, NRI net reclassification index.
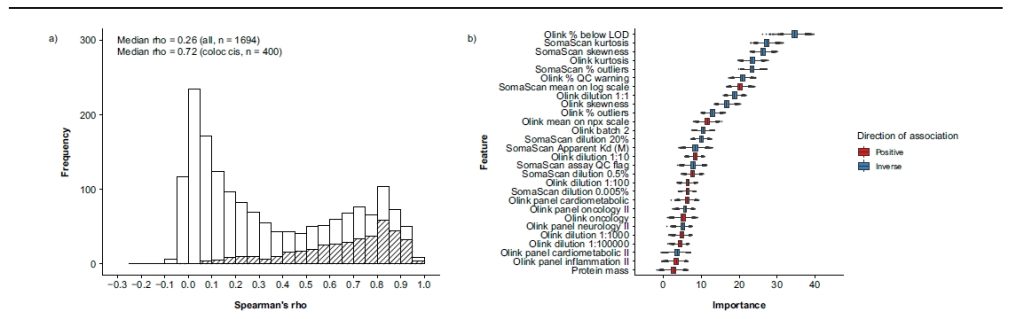
Fig. 2 | Observational correlations, associated factors, and comparison of pQTLs for 1694 proteinsmeasured using both Olink and SomaScan platforms. Analyses were conducted for 1694 matched proteins among 3976 participants. a Observational correlations between Olink and SomaScan, with shaded areas indicating proteins with colocalising cis-pQTLs. b Features predictive of Spearman’s rho and their importance in Boruta feature selection. 28 of 87 features were selected by Boruta with p values < 0.01 (two-sided). Importance measures represent Z-scores of mean decrease accuracy measure with normalised permutation. The centre, bounds, and whiskers of boxes represent themedian, first/third quartile, and 1.5 times the interquartile range of the data.
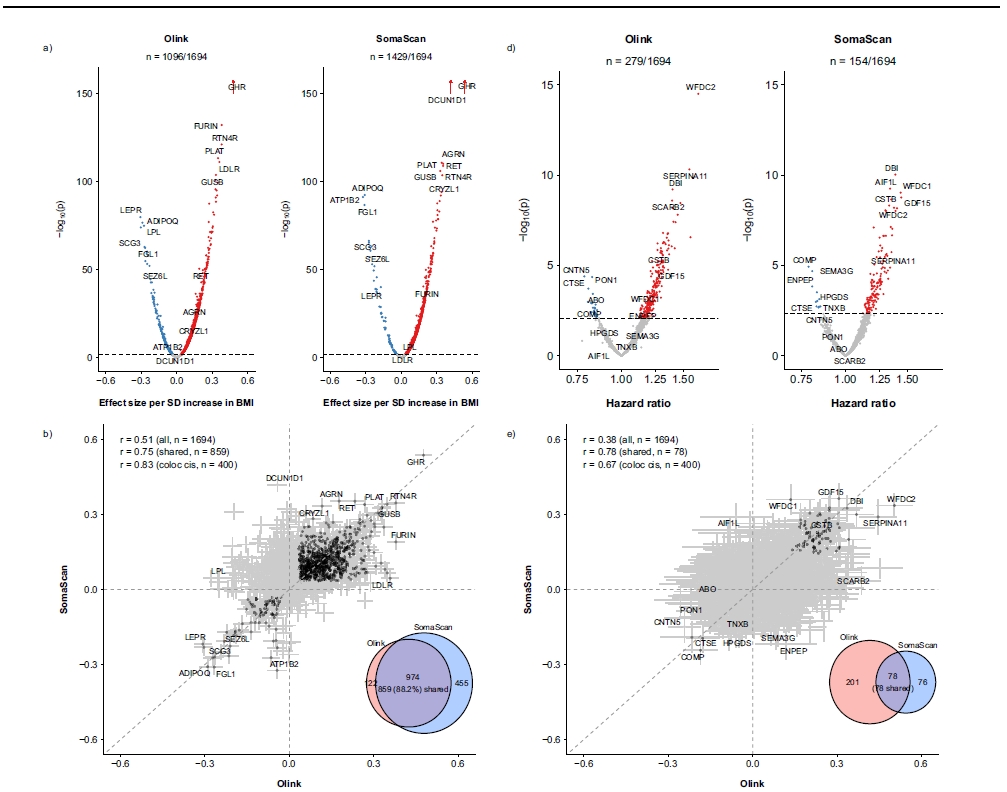
Fig. 3 | Comparison ofnumber of proteins significantly associatedwith BMI and risk of incident IHD and their effect sizes between Olink and SomaScan platforms. Analyses were conducted for 1694 matched proteins among 3976 participants, including 1951 IHD cases and 2025 subcohort participants. a Associations between protein levels and BMI, with coloured dots indicating significant associations. b Comparison of effect sizes (beta coefficients) for associations with BMI, with darker dots indicating significant associations and error bars indicating 95% confidence intervals. d Associations between protein levels and IHD. e Comparison of effect sizes (beta coefficients) for associations with IHD, with darker dots indicating significant associations and error bars indicating 95%confidence intervals.
4. 疾病风险预测能力
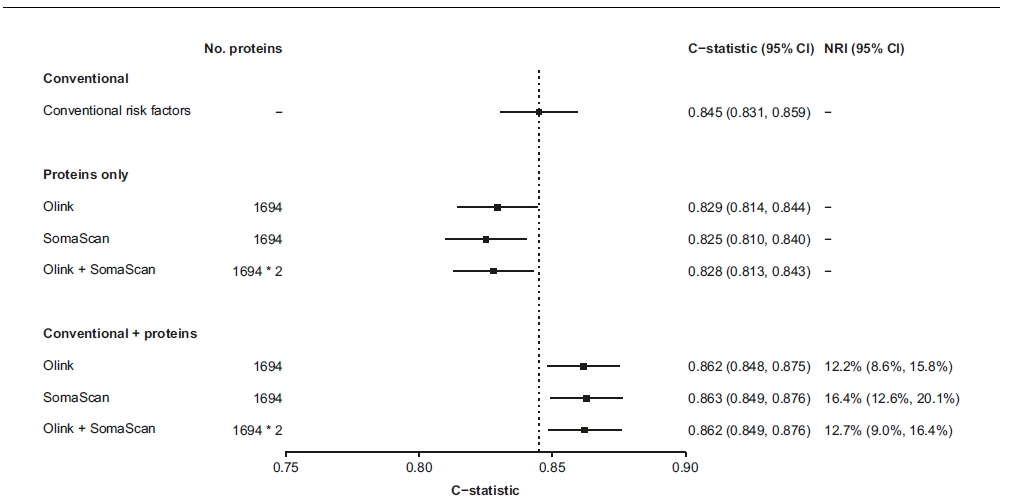
风险预测模型:仅用蛋白组数据预测IHD的C-statistic略低于传统风险因子模型(Olink: 0.829 vs 0.845),但蛋白组与传统因子联合后,C-statistic显著提升(Olink: 0.862,SomaScan: 0.863),NRI分别为12.2%和16.4%。
Fig. 4 | Performance of proteins measured using Olink and SomaScan platforms for prediction of incident IHD. Analyses were conducted for 1694 matched proteins among 3976 participants, including 1951 IHD cases and 2025 subcohort participants. Conventional risk factors for cardiovascular disease included age, sex, smoking, type 2 diabetes, systolic blood pressure, and waist circumference. Protein measurements for 1694 one-to-one matched proteins from both platforms or from one platform were used to build the models. Data are presented as estimated C-statistics, with error bars indicating 95% confidence intervals. NRI were computed with a decile-based method. IHD ischaemic heart disease, NRI net reclassification index.
Reference: Wang, B., Pozarickij, A., Mazidi, M. et al. Comparative studies of 2168 plasma proteins measured by two affinity-based platforms in 4000 Chinese adults. Nat Commun16, 1869 (2025). https://doi.org/10.1038/s41467-025-56935-2